Glaucoma
What is Glaucoma?
Glaucoma refers to a category of eye disorders often associated with increased intraocular pressure which can damage destroys the nerve cells in the retina and optic nerve of the eye.
Although raised intraocular pressure is a significant risk factor for developing glaucoma, there is no set threshold for intraocular pressure that causes glaucoma. One person may develop nerve damage at a relatively low pressure, while another person may have high eye pressure for years and yet never develop damage.
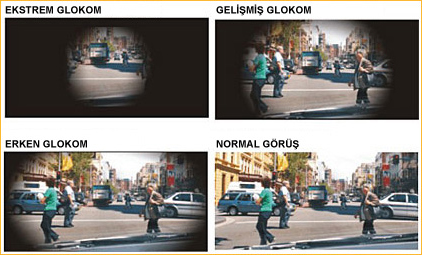
Sometimes called the silent thief of sight, glaucoma can damage your vision so gradually you don't notice any loss of vision until the disease is at an advanced stage. In contrast to glaucoma, in ocular hypertension the pressure is not high enough to cause optic nerve damage and vision loss. About 2% of the population ages 40-50 and 8% over 70 have elevated intraocular pressure.
Glaucoma is one of the leading cause of blindness in the developed countries.
Glaucoma is not curable and vision lost cannot be regained. With medication and/or surgery, it is possible to halt further loss of vision. Since glaucoma is a chronic condition, it must be monitored for life. Everyone is at risk for glaucoma from babies to senior citizens. Older people are at a higher risk for glaucoma but babies can be born with glaucoma.
Because most people with glaucoma have no early symptoms or pain from this increased pressure, it is important to see your ophthalmologist regularly so that glaucoma can be diagnosed and treated before long-term visual loss occurs.
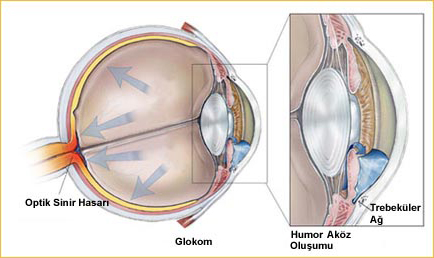
The major risk factor for most glaucomas is increased intraocular pressure. Intraocular pressure is a function of production of liquid aqueous humor by the ciliary body of the eye and its drainage through the trabecular meshwork. Aqueous humor flows from the ciliary bodies into the posterior chamber. It then flows through the pupil of the iris into the anterior chamber. From here the trabecular meshwork drains aqueous humor via canal into general blood circulation.
What are the different types of Glaucoma?
There are two main types of glaucoma which are open angle glaucoma and angle closure glaucoma.
In primary open-angle glaucoma, the drainage angle formed by the cornea and the iris remains open, but the microscopic drainage channels in the angle called the trabecular meshwork are partially obstructed, causing the aqueous humor to drain out of the eye too slowly. This leads to fluid backup and a gradual increase of pressure within your eye. The exact cause of primary open-angle glaucoma remains unknown.
In angle-closure glaucoma, the iris bulges forward to narrow or block the drainage angle formed by the cornea and the iris. As a result, aqueous fluid can no longer access the trabecular meshwork at the angle, so the eye pressure increases abruptly. Angle-closure glaucoma usually occurs suddenly (acute angle-closure glaucoma), but it can also occur gradually (chronic angle-closure glaucoma.) There is also secondary glaucoma refers to any case in which another disease such as eye injury, cataract formation, diabetes or steroid usage causes or contributes to increased eye pressure, resulting in optic nerve damage and vision loss, as well.
Congenital glaucoma is the other group which presents at birth and mostly are diagnosed during the first year of life. Sometimes symptoms are not recognized until later in infancy or early childhood.
Another form of the disease, poorly understood but not uncommon, is low-tension glaucoma. In this form, optic nerve damage occurs even though eye pressure stays within the normal range. Why this happens is unknown. Some experts believe that people with low-tension glaucoma may have an abnormally sensitive optic nerve or a reduced blood supply to the optic nerve caused by atherosclerosis.
Chronic open-angle glaucoma is the most common form of glaucoma in the United States. Typically, open-angle glaucoma has no symptoms in its early stages and vision remains normal. Unfortunately, two-thirds of those with closed-angle glaucoma develop it slowly without any symptoms warning an acute attack might be coming.
Some people are born with the iris too close to the drainage angle. In these eyes the iris can be sucked into the drainage angle and block it completely. Since the fluid cannot exit the eye, pressure inside the eye builds rapidly and causes an acute closed-angle attack. Blurry vision, severe eye pain, headache, halos aroun light, nausea and vomiting are the symptoms of closed-angle glaucoma. This is a true eye emergency. Unless this type of glaucoma is treated quickly, blindness can result.
The most important risk factors for glaucoma include
• Age (60 years and older)
• Elevated eye pressure
• Family history of glaucoma
• Farsightedness or nearsightedness
• Past eye injuriesSteroid use
• Other health problems like diabetes or migraine headaches.
How are glaucoma patients diagnosed and followed up?
The optic nerve is made up of many nerve fibers that carry images to the brain. It's like an electric cable containing numerous wires. When glaucoma damages the optic nerve fibers, blind spots develop. If the entire nerve is destroyed, blindness results.
Regular eye examinations by an ophthalmologist are the best way to detect glaucoma. Of the following five common tests for glaucoma, the first two are routine. The tonometry test measures the inner pressure of the eye. Usually drops are used to numb the eye. Then the doctor or technician will use a special device that measures the eye's pressure.
Ophthalmoscopy is used to examine the inside of the eye, especially the optic nerve. In a darkened room, the doctor will magnify your eye by using an ophthalmoscope.
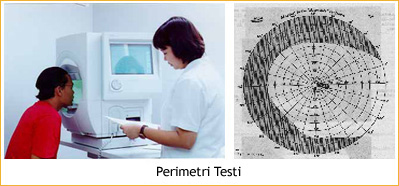
The perimetry test is also called a visual field test. During this test, you will be asked to look straight ahead and then indicate when a moving light passes your peripheral vision. This helps draw a map of your vision.
 The gonioscopy is a painless eye test that checks if the angle where the iris meets the cornea is open or closed, showing if either open angle or closed angle glaucoma is present.
Optical coherence tomography (OCT) is a non-invasive examination that uses light waves to visualize the retina and the optic nerve. Damage to optic nerve fibers can be detected early by OCT.
The gonioscopy is a painless eye test that checks if the angle where the iris meets the cornea is open or closed, showing if either open angle or closed angle glaucoma is present.
Optical coherence tomography (OCT) is a non-invasive examination that uses light waves to visualize the retina and the optic nerve. Damage to optic nerve fibers can be detected early by OCT.
These tests may need to be repeated if any changes in your condition is suspected.
What is the treatment of Glaucoma?
Treatment can prevent vision loss, but as a rule damage caused by glaucoma is irreversible.
Depending upon the type of glaucoma, treatment may include medication, usually prescription eyedrops, or surgery to lower the pressure in the eye and prevent further damage to the optic nerve. While there is no cure as yet for glaucoma, early diagnosis and continuing treatment can preserve eyesight.
Glaucoma is usually controlled with eyedrops taken daily. These medications lower eye pressure, either by decreasing the amount of fluid produced within the eye or by improving the flow through the drainage angle.
While these medications can preserve your vision, they may also have side effects. Some eyedrops may cause stinging, itching, red eyes, redness of the skin around the eyes, changes in pulse and heartbeat, changes in breathing (especially with asthma or emphysema), dry mouth, changes in sense of taste, headaches, blurred vision or change in eye color. A patient should tell the ophthalmologist if he experiences side effects. Also other medications can interact with other medications. Therefore, it is important that patient make a list of the medications he takes regularly.
Surgery involves either laser treatment or making a cut in the eye to reduce the intraocular pressure which is named filtering microsurgery.
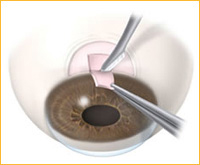
Doctors often recommend laser surgery before filtering microsurgery, unless the eye pressure is very high or the optic nerve is badly damaged. During laser surgery, a tiny but powerful beam of light is used to make several small scars in the eye’s trabecular meshwork which is the drainage system. The scars help increase the flow of fluid out of the eye. During the laser surgery, the eye is numbed so that there is little or no pain.
In contrast, filtering microsurgery involves creating a drainage hole in the sclera with the use of a small surgical tool. The new drainage hole allows fluid to flow out of the eye and helps lower eye pressure. This procedure is called a trabeculectomy or a sclerostomy. This filtering surgery is successful in about 70-90% of cases, for at least one year. Occasionally, the surgically-created drainage hole begins to close and the pressure rises again. This happens because the body tries to heal the new opening in the eye. This rapid healing occurs most often in younger people, because they have a stronger healing system. Anti-wound healing drugs can help slow down the healing of the opening. If needed, glaucoma filtering surgery can be done a number of times in the same eye.
Acute angle-closure glaucoma is an ocular emergency that requires immediate treatment to lower the high intraocular pressure. If the pressure doesn’t decrease with drug therapy, laser iridotomy or surgical peripheral iridectomy must be performed promptly to save the patient’s vision.
Last Updated: October 23, 2024


























